Creatine: The Complete Evidence-Based Guide (2026)
Creatine is the most-studied supplement in sports nutrition history. More than 1,000 peer-reviewed papers have examined its effects on strength, lean mass, recovery, and — more recently — the brain, making it one of the few ingredients in the supplement aisle where the science genuinely outpaces the marketing (Kreider et al., 2017). Yet despite that mountain of evidence, most consumers still get their creatine information from product labels and forum threads.
This guide cuts through that noise. By the end, you’ll know exactly what creatine does inside your body, which form is worth your money, the right dose for your goals, when to take it, and which side effects are actually supported by data — versus which ones are gym-bro folklore that refuses to die.
Every claim here is anchored to peer-reviewed literature: meta-analyses, systematic reviews, randomized controlled trials, and the most recent position stands from the International Society of Sports Nutrition. Where the evidence is strong, we say so plainly. Where it’s preliminary, we flag it. No hype, no hedging.
What Creatine Actually Is
Creatine is a nitrogen-containing compound your body assembles from three amino acids — arginine, glycine, and methionine. Your liver, kidneys, and pancreas produce roughly 1 gram per day on their own, and about 95% of the creatine in your body is stored inside skeletal muscle as a molecule called phosphocreatine (Kreider et al., 2017).
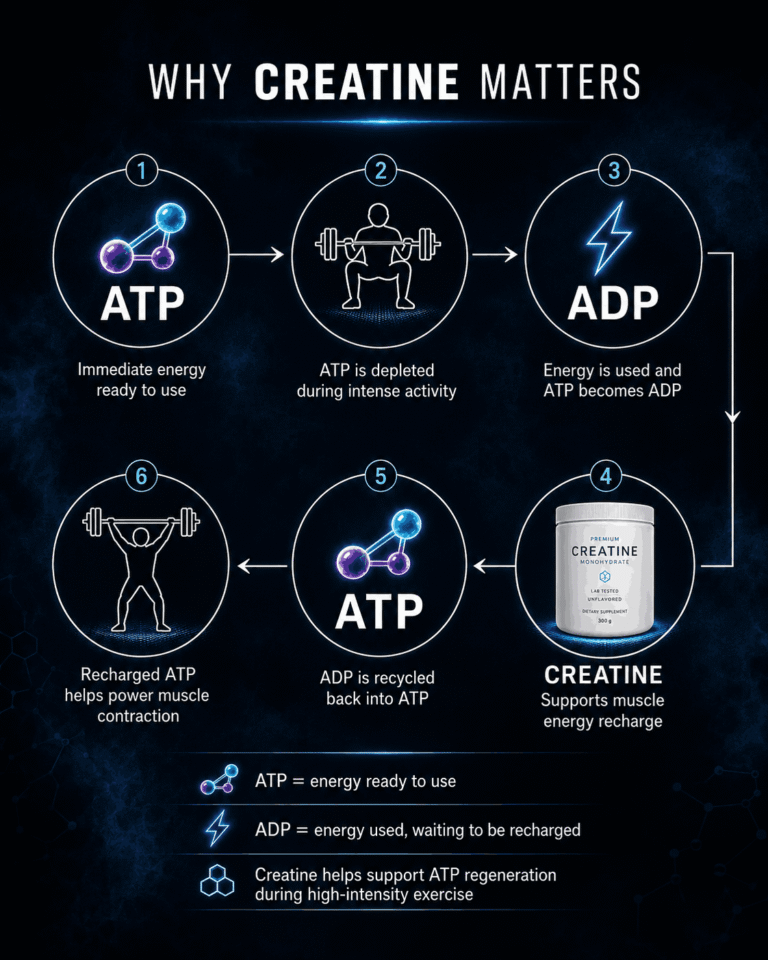
Phosphocreatine functions as a rapid-deployment energy reserve. When your muscles need to contract explosively — a heavy single, a 40-yard sprint, a max-effort jump — they burn through ATP (the cell’s energy currency) in seconds. Phosphocreatine donates a phosphate group to regenerate ATP almost instantly, keeping your output high for a few more seconds before slower energy systems take over. More phosphocreatine in the tank means more quality reps, more sprints, more total work in the same session.
Your second source of creatine is food. Animal flesh is essentially the only meaningful dietary contributor:
- Herring: ~3–4.5 g per pound (the highest natural source)
- Beef and pork: ~2–2.5 g per pound
- Salmon and tuna: ~1.5–2 g per pound
- Plant foods: trace amounts only
This dietary reality is why vegetarians and vegans walk around with measurably lower muscle creatine stores than omnivores — typically 20–30% lower at baseline — and, as you’ll see in the benefits section, why they tend to be the largest responders when they start supplementing (Burke et al., 2003).
Why Your Body’s Natural Creatine Isn’t Enough for Performance
Here’s the part most articles skip: your muscles can hold significantly more creatine than they normally store. A typical untrained adult walks around at roughly 60–80% of maximum saturation. To eat your way to a full tank, you’d need to put down something like two pounds of raw beef every single day — and cooking destroys a meaningful fraction of dietary creatine before it ever reaches your plate.
In our reading of the literature, this is the single most under-explained point in mainstream creatine content. Supplementation isn’t about adding something exotic to your physiology. It’s about topping up a reservoir your body already uses every time you train hard, but almost never fills from food alone. A consistent 3–5 g daily dose closes that gap — and, as the rest of this guide will show, the downstream effects on strength, recovery, and even cognition are some of the best-documented in all of sports science.
How Creatine Works (Mechanism)
To understand why creatine moves the needle on performance, you have to understand the energy system it plugs into — the phosphocreatine (PCr) system, also called the ATP-PCr system or the immediate energy system.
Every muscle contraction in your body is paid for in ATP (adenosine triphosphate). When a muscle fires, ATP loses a phosphate group, becomes ADP, and releases energy. The problem is that your muscles only store enough free ATP to fuel about 1 to 2 seconds of maximum effort. After that, you need to regenerate ATP from ADP or the contraction stops.
This is where phosphocreatine earns its keep. Stored alongside ATP inside the muscle cell, PCr donates its phosphate group directly to ADP to instantly rebuild ATP — no oxygen, no glucose, no waiting. The handoff is so fast it’s measured in milliseconds, and it extends your maximum-effort window to roughly 8 to 12 seconds before slower energy systems (glycolysis, then aerobic metabolism) take over (Kreider et al., 2017).
That window is exactly where strength and power training lives: a heavy triple, a 30-meter sprint, a max vertical jump, the explosive portion of a clean. More phosphocreatine in the tank means a higher ceiling on those efforts and faster recovery between sets, which over weeks of training translates to more total work performed — and more total work is the engine of adaptation.

There’s a second mechanism worth understanding, because it explains why creatine produces gains that go beyond what raw energy availability alone would predict. Creatine is osmotically active — it pulls water into the muscle cell with it. This cell volumization effect is the source of the “fuller” look lifters notice within a couple of weeks, and it’s not the same as bloating (which sits under the skin, not inside the muscle).
The interesting part is what happens downstream of that swelling. Increased cellular hydration appears to act as an anabolic signal in its own right, upregulating protein synthesis pathways and satellite cell activity — the cells responsible for muscle repair and growth (Kreider et al., 2017). In plain terms: a well-hydrated muscle cell is a more anabolically receptive muscle cell. This is part of why creatine reliably produces lean mass gains on top of strength gains, not just one or the other.
Beyond Muscle: Emerging Research on Cognitive Function
Your brain is the most energy-hungry organ you own. It accounts for roughly 2% of your body weight but burns about 20% of your daily energy expenditure, and like muscle tissue, neurons rely on the ATP-PCr system to handle sudden demands. It shouldn’t be surprising, then, that researchers have started asking what happens when you increase brain creatine stores.
A 2018 meta-analysis pooling six randomized trials found that creatine supplementation produced measurable improvements in short-term memory and reasoning, with the largest effects seen in vegetarians and older adults — the two groups that start out with the lowest baseline creatine levels (Avgerinos et al., 2018). More recently, a 2024 study in Scientific Reports showed that a single high dose of creatine partially reversed the cognitive deficits caused by 21 hours of sleep deprivation, alongside measurable changes in the brain’s high-energy phosphate metabolism (Gordji-Nejad et al., 2024).
We’d file the cognitive evidence under promising but early. The signal is real, especially in stressed or depleted states (sleep deprivation, low baseline stores, aging), but the studies are still small and the protocols vary widely. Anyone telling you creatine is a guaranteed nootropic is overselling. Anyone telling you it has no effect on the brain is behind on the literature.
Proven Benefits of Creatine (Evidence-Weighted)
“Creatine works” is one of those statements that’s technically true but practically useless. Works for what, by how much, and how confident are we — those are the questions that actually matter when you’re deciding whether to buy a tub. Below is our evidence-weighted breakdown of every benefit creatine is currently claimed to deliver, ranked by the quality and quantity of human trials supporting it.
The star rating reflects evidence strength: ★★★★★ means decades of replicated RCTs and meta-analyses, ★ means a single study or mechanistic speculation with little human data behind it. Effect sizes are pulled directly from the cited research where possible.
| Benefit | Evidence Level | Effect Size |
|---|---|---|
| Strength gains | Strong | ~8% greater than training alone |
| Lean mass | Strong | +1–2 kg over 4–12 weeks |
| Power output | Strong | Significant in repeated sprint protocols |
| Sarcopenia (elderly) | Good | +1.4 kg lean mass when combined with resistance training |
| Cognitive function | Moderate | Strongest in vegetarians, elderly, and sleep-deprived states |
| Bone density | Early | Limited human trials, mostly in postmenopausal women |
| Hair loss prevention | Insufficient | No human RCTs; mechanistic speculation only |
Strength and Lean Mass: The Original Use Case
The strongest evidence for creatine sits exactly where most people use it: putting more weight on the bar and more muscle on the frame. A foundational meta-analysis by Rawson and Volek synthesized 22 controlled studies and found that subjects supplementing creatine alongside resistance training gained roughly 8% more strength on average than those doing the same training without it — a substantial edge that compounds over months and years (Rawson & Volek, 2003).
The lean mass story is just as consistent. Across dozens of trials, supplementing 3–5 g daily during a structured training program reliably produces an extra 1 to 2 kilograms of lean body mass over 4–12 weeks versus training alone (Kreider et al., 2017). Part of that is true muscle protein accretion; part is the cell volumization effect described earlier. Either way, the scale moves and the mirror agrees — which is more than can be said for most supplements that claim to do the same thing.
Power Output and Repeated Sprint Performance
For sports and training protocols that involve repeated short bursts — interval running, team sports, CrossFit-style metcons, combat sport drills — creatine produces particularly clean improvements. Because the phosphocreatine system recharges between efforts, athletes with more saturated muscle stores can hit a higher output on the second, third, and fourth sprint of a set, where unsaturated athletes fade. A 2003 meta-analysis covering 96 studies confirmed significant improvements in repeated-bout work capacity across nearly every sport type tested (Branch, 2003).
Sarcopenia: Creatine for Aging Adults
One of the most underrated applications of creatine has nothing to do with the gym demographic that buys it. Sarcopenia — the age-related loss of muscle mass and strength — affects most adults past 60, and it’s a strong predictor of falls, fractures, and loss of independence. Meta-analyses of older adults have shown that combining creatine supplementation with resistance training produces meaningfully greater gains in lean mass and functional strength than resistance training alone (Devries & Phillips, 2014). This is one of the cleanest cost-benefit interventions available for healthy aging, and it remains badly under-recommended outside sports nutrition circles.
The benefits at the bottom of the table — bone density, hair loss prevention, and a handful of more speculative claims — are where you should calibrate your expectations downward. We cover the safety side of the hair loss question specifically in Section 6, because the myth has more legs than the evidence behind it.
Types of Creatine — What Actually Matters
Walk into any supplement store and you’ll find a dozen creatine variants, each with its own marketing pitch: faster absorption, no bloat, no loading needed, “advanced delivery.” Most of them exist because monohydrate is so cheap and so out-of-patent that brands need a premium-priced angle to sell. Here’s what the research actually says about each form.
Creatine Monohydrate
This is the original — the form used in the overwhelming majority of the 1,000+ creatine studies ever published. When researchers say “creatine works,” they almost always mean monohydrate works. It’s stable on the shelf, dissolves in water (especially in micronized form), absorbs near-completely when taken with a normal meal, and costs a fraction of every alternative on the market. The International Society of Sports Nutrition’s official position is that monohydrate remains “the most effective ergogenic nutritional supplement currently available to athletes” — and they specifically name monohydrate, not the alternatives (Kreider et al., 2017).
Creatine HCL (Hydrochloride)
Marketed primarily on the claim that it dissolves better and causes less gastrointestinal discomfort or “bloat.” The solubility claim is technically true in a glass of water. The translation to actual outcomes — strength, lean mass, performance — has never been demonstrated to be superior to monohydrate in a head-to-head human trial. You’re paying 3–5x the per-gram price for a marketing differentiation, not a measured advantage.
Creatine Ethyl Ester
Sold for years as a “more bioavailable” form that supposedly bypassed monohydrate’s absorption issues — issues that didn’t really exist in the first place. A 2009 study from Spillane and colleagues compared ethyl ester directly against monohydrate over 47 days of training and found ethyl ester was actually less effective at raising muscle creatine levels, with no advantage in strength or body composition (Spillane et al., 2009). Skip it.
Buffered Creatine (Kre-Alkalyn)
The pitch is that buffering creatine to a higher pH prevents its breakdown into creatinine in the stomach, making smaller doses more effective. A 28-day controlled trial directly compared Kre-Alkalyn against standard monohydrate and found no superiority on any measured outcome — muscle creatine content, strength, or body composition — at either equivalent or lower doses (Jagim et al., 2012). The premium price isn’t buying you a better product.
Liquid Creatine
Pre-dissolved creatine in liquid form sounds convenient, but creatine in solution degrades into creatinine — an inactive waste product — within days to weeks depending on pH and temperature. By the time a liquid creatine product reaches your shelf, a meaningful fraction of the active compound is already gone. Avoid.
Creatine Magnesium Chelate
One of the few alternatives with a single decent study showing performance comparable to monohydrate, on the theory that magnesium aids ATP regeneration. “Comparable” is the operative word — not superior — and the cost premium puts it firmly in the “interesting but unnecessary” category for most users.
The Verdict
After thirty years of comparison studies, no creatine variant has demonstrated a consistent, replicated advantage over plain monohydrate on the outcomes that actually matter: more strength, more muscle, better performance. Monohydrate wins on cost, evidence, and effectiveness. Every other form is either equivalent at best (and more expensive) or measurably worse.
If you want a deeper side-by-side on the two forms people ask about most, we break it down in our Creatine Monohydrate vs. HCL comparison. Otherwise, the practical takeaway is simple: buy monohydrate, ideally from a brand that uses Creapure® (a German-manufactured, third-party-tested raw material we cover in Section 8) and don’t overthink it. A handful of brands consistently meet that bar — we maintain an updated shortlist in our tested picks for best creatine monohydrate.
Dosing & Timing
The dosing protocol for creatine is one of the most-debated and least-complicated topics in supplementation. Decades of research have converged on a small set of clear answers, and most of the disagreement you’ll see online is about edge cases that don’t meaningfully affect outcomes. Here’s the practical playbook.
Loading Phase vs. No Loading
There are two valid ways to saturate your muscle creatine stores:
| Protocol | Daily Dose | Time to Full Saturation |
|---|---|---|
| Loading phase | 20 g/day (split into 4 × 5 g doses) for 5–7 days, then 3–5 g/day maintenance | ~1 week |
| No loading | 3–5 g/day from day one | ~3–4 weeks |
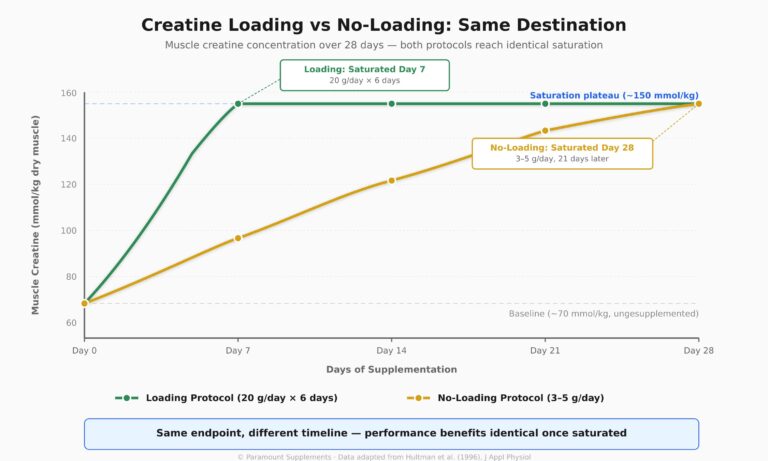
Both protocols end up in exactly the same place: a fully saturated muscle creatine pool that delivers the full performance benefit. Loading just gets you there faster. The original Hultman study that established the loading protocol back in 1996 showed that 20 g/day for 6 days raised muscle creatine to the same plateau that 3 g/day reached after 28 days (Hultman et al., 1996).
The practical question is whether saving three weeks is worth the small downside of loading: some people experience mild GI discomfort or temporary water-weight gain when consuming 20 g per day. If you’re prepping for a specific event or just impatient, load. If you’re playing the long game, skip it. We dig deeper into when loading actually pays off in our breakdown of the loading phase: myth or necessary?
When to Take Creatine: Pre vs. Post-Workout
This is the question that generates the most forum debate and the least real-world impact. The most-cited trial on the topic — Antonio and Ciccone in 2013 — split recreational bodybuilders into pre-workout and post-workout creatine groups and tracked them for four weeks. The post-workout group showed a slight edge in body composition and strength outcomes, but the differences were small and the authors emphasized that consistency mattered far more than timing (Antonio & Ciccone, 2013).
The practical translation: if you can take it post-workout, do that. If your routine works better pre-workout, do that instead. The single biggest predictor of whether creatine works for you is whether you take it every day, not which side of your training session you take it on.
Rest Days: Take It or Skip It?
Take it. The whole point of consistent daily dosing is keeping your muscle creatine pool saturated — and saturation isn’t tied to whether you train that day. Skipping creatine on rest days is one of those folk-wisdom habits that has zero supporting evidence and slowly chips away at the saturation you spent weeks building.
With Food, Insulin, and Carbs
Co-ingesting creatine with carbohydrates and protein produces a small bump in muscle uptake, likely mediated by insulin’s effect on creatine transport into the cell. The effect is real but modest, and absolutely not required for the supplement to work. Take your creatine with whatever meal, shake, or glass of water is most convenient. Don’t engineer your day around it.
Side Effects & Safety
Creatine is one of the most extensively safety-tested supplements on the market. Controlled trials lasting up to five years in healthy populations have repeatedly failed to identify clinically meaningful adverse effects at standard doses — which is more than most products in your kitchen can claim (Kreider et al., 2017). That said, the supplement does come with a handful of real side effects, plus a much longer list of imagined ones that refuse to die in gym conversation. Here’s what the evidence says about both.
Water Retention: Real, But Not What You Think
Creatine pulls water into the muscle cell. This is real, measurable, and the source of most “I gained 2 kg in the first week” reports during a loading phase. But this water sits inside muscle tissue — not under the skin — which means it looks like fullness and round muscle bellies, not the puffy, smoothed-over look of subcutaneous water retention. Most lifters consider this a feature, not a side effect.
Kidney Concerns: Persistently Wrong
The kidney rumor has been studied to death and consistently debunked in healthy individuals. Poortmans and Francaux’s foundational 2000 review found no evidence of renal dysfunction in long-term creatine users with normal kidney function (Poortmans & Francaux, 2000), and follow-up work by Kim and colleagues reached the same conclusion across multiple controlled trials (Kim et al., 2011). The misunderstanding usually starts with creatinine — a creatine byproduct that appears slightly elevated on standard lab tests in supplemented individuals. Elevated creatinine in a creatine user is metabolic, not pathological, and a knowledgeable clinician will recognize the difference.
Hair Loss and DHT: One Study, No Replication
The hair loss claim traces to a single 2009 trial in college rugby players, which found a roughly 56% increase in the DHT-to-testosterone ratio after creatine loading (Van der Merwe et al., 2009). Here’s the critical part most articles skip: the study did not measure hair loss. It measured a hormone associated with hair loss in genetically susceptible individuals. In the 15+ years since publication, no study has replicated the DHT finding, and no controlled trial has shown a direct link between creatine and hair shedding. The myth has more longevity than the evidence behind it.
Cramping and Dehydration
The intuition that “creatine pulls water into muscle, therefore creatine causes dehydration” runs backwards. In practice, studies of athletes training in heat — including a season-long study of college football players — have shown that creatine users experience the same or fewer cramping incidents than non-users (Greenwood et al., 2003). Stay hydrated as you normally would and there’s nothing here to engineer around.
For a deeper look at every side effect that’s been formally studied, see our breakdown of creatine side effects: what 50+ studies show.
Who Should Take Creatine
The benefits of creatine aren’t evenly distributed across the population. Some groups see large, fast, obvious gains. Others see modest improvements that compound over years. A few populations barely respond at all. Here’s how the evidence breaks down:
Resistance Trainers
The clearest yes in the entire literature. If you train with weights and your goal is more strength, more muscle, or more work capacity in the gym, creatine is the highest-confidence supplement intervention available — roughly an 8% strength advantage over the same training without it (Rawson & Volek, 2003).
Endurance Athletes
Mixed evidence. Pure aerobic endurance (marathon running, long-distance cycling) shows little to no improvement, because the phosphocreatine system isn’t the rate-limiting factor. But if your sport involves repeated sprints, climbs, or interval-style efforts — soccer, rugby, CrossFit, MMA, tennis — the carryover from improved repeat-effort capacity is direct and meaningful.
Vegetarians and Vegans
The largest responders in nearly every study that measures baseline diet. Because plant-based eaters start with 20–30% lower muscle creatine stores, they have more headroom to fill — and the effect sizes for strength, cognition, and recovery tend to be largest in this group (Burke et al., 2003).
Older Adults
One of the highest-leverage uses of creatine, and badly under-recommended outside sports nutrition circles. Combined with resistance training, supplementation produces meaningfully greater gains in lean mass, strength, and functional performance in adults over 60 than training alone (Devries & Phillips, 2014). For sarcopenia prevention, this is among the safest, cheapest, and most evidence-backed interventions available.
Women
Same dosing, same benefits, fewer products marketed to them. Smith-Ryan and colleagues published a comprehensive 2021 review confirming that creatine works as effectively in women as in men across the lifespan, with particular value during peri-menopause and post-menopause when both lean mass and bone density become clinical priorities (Smith-Ryan et al., 2021).
Teens
Controlled trials in adolescent athletes have shown the same safety and efficacy profile as in adults at standard doses. That said, this is a population where parental judgment, coach involvement, and a food-first approach deserve the first word. Creatine isn’t a substitute for sleep, training fundamentals, and adequate dietary protein at any age — and especially not during adolescence.
How to Choose a Quality Creatine
The good news is that creatine monohydrate is a commodity ingredient — chemically identical from one quality manufacturer to the next. The less-good news is that not all manufacturers are quality. A small but real percentage of products on the market contain impurities, lower-than-advertised creatine content, or unnecessary fillers hidden inside proprietary blends. Here’s what to look for on the label:
Creapure® Designation
Creapure® is creatine monohydrate manufactured by AlzChem in Germany, and it’s the most rigorously purity-tested raw material in the category. Independent batch testing for known contaminants (creatinine, dicyandiamide, dihydrotriazine) is standard. If the label says “Made with Creapure®,” you’ve eliminated the vast majority of quality concerns in a single glance.
Third-Party Certification
Look for Informed Sport, NSF Certified for Sport, or USP Verified marks on the tub. These programs test for banned substances and label accuracy, and they matter especially if you’re a competing athlete subject to drug testing — but they’re a useful trust signal for any consumer.
No Proprietary Blends
Avoid any product that lists “creatine matrix,” “advanced creatine complex,” or any other phrase that hides specific ingredient amounts behind a single total. You should be able to see the exact creatine monohydrate dose per serving on the label, full stop. If it’s hidden, it’s hidden for a reason.
Micronized vs. Standard
Micronized creatine has been milled to a finer powder, which improves how well it dissolves in water. It’s not “better” creatine — same molecule, same effect — just less gritty in your glass. Worth the marginal price difference if you mix yours in water; irrelevant if you take it with a thicker shake or smoothie.
Skip the Marketing Theater
“Advanced delivery system.” “Time-released.” “Enhanced bioavailability matrix.” If a creatine product is selling you a delivery mechanism rather than the dose, you’re paying for marketing copy, not for science. Plain monohydrate at 3–5 g per serving is what 1,000+ studies have validated. Anything more elaborate is a story, not a product.
Frequently Asked Questions
How long does creatine take to work?
Without a loading phase, expect noticeable strength and performance benefits in 2–4 weeks as your muscle creatine stores reach full saturation. With a loading phase (20 g/day for a week), the same effects typically show up within 7–10 days. The cell volumization effect — the “fuller” muscle appearance — often appears first, sometimes within the first few days.
Should I cycle creatine?
No. There’s no evidence that cycling creatine improves results or reduces any side effects, and stopping causes muscle creatine stores to fall back to baseline over 4–6 weeks. The continuous daily dosing protocol used in nearly every long-term safety and efficacy study is also what works best for sustained performance.
Can I mix creatine with coffee?
Yes. Older claims that caffeine cancels out creatine’s effects came from a small 1996 study that hasn’t been replicated, and more recent research shows no meaningful interference. Mixing your 3–5 g dose into your morning coffee is fine if it helps you remember to take it consistently — and consistency is the single biggest predictor of results.
Is creatine a steroid?
No. Creatine is a nitrogen-containing organic compound produced naturally by your liver, kidneys, and pancreas, and obtained from red meat and fish. It’s not a hormone, not chemically related to anabolic steroids, and works through an entirely different mechanism — boosting the muscle’s energy regeneration system rather than altering hormone levels.
Does creatine cause acne?
There’s no clinical evidence linking creatine to acne. The association in gym folklore likely reflects a confound: people who start creatine often start training harder, eating more, and sweating more — all of which can independently affect skin. Creatine itself has no documented effect on sebaceous gland activity or sebum production.
What happens if I stop taking creatine?
Muscle creatine stores gradually return to baseline over 4–6 weeks, and the small performance edge fades along with them. You won’t lose the muscle you built — those gains were real training adaptations that don’t depend on creatine to persist — but the extra ceiling on strength and repeat-effort work capacity will go away until you resume supplementation.
Can I take creatine on an empty stomach?
Yes, with one small caveat. Some people experience mild stomach discomfort taking 5 g of creatine on a completely empty stomach, especially during a loading phase when total daily intake hits 20 g. If that’s you, take it with food, milk, or a shake. The supplement absorbs effectively either way.
Does creatine expire?
In powder form, creatine monohydrate is exceptionally stable. Stored properly — sealed, dry, at room temperature — it remains effective well past most printed expiration dates. The reason liquid creatine is a poor choice is exactly this: once dissolved in water, creatine degrades into inactive creatinine within days to weeks.
What brand of creatine do you recommend?
We don’t endorse a single “best” brand, because formulation quality, third-party testing status, and per-gram pricing all shift over time. Instead, we maintain a regularly updated shortlist of products that meet our quality criteria — Creapure® sourcing or independent purity testing, transparent labels, no proprietary blends. See our current top picks here.
The Bottom Line
Creatine monohydrate is one of the rare supplements where the consumer marketing has actually caught up to the science — and the science has been remarkably consistent for three decades. It builds strength. It builds lean mass. It improves repeat-effort performance. It’s safe at standard doses for the overwhelming majority of healthy users. It costs almost nothing per gram. And the emerging cognitive research, while still preliminary, is among the most interesting frontiers in supplementation today.
If you’ve made it to this paragraph, you now know more about creatine than most personal trainers, supplement retailers, and a meaningful fraction of medical professionals. The next step is simple: pick a quality monohydrate product, take 3–5 grams daily, and let the saturation do its quiet work. We maintain a tested, third-party-verified shortlist of products that meet our quality criteria — see our top picks for best creatine monohydrate in 2026.
References
- Kreider RB, Kalman DS, Antonio J, et al. (2017). International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. Journal of the International Society of Sports Nutrition, 14:18. PMID: 28615996
- Rawson ES, Volek JS (2003). Effects of creatine supplementation and resistance training on muscle strength and weightlifting performance. Journal of Strength and Conditioning Research, 17(4):822–831. PMID: 14636102
- Antonio J, Ciccone V (2013). The effects of pre versus post workout supplementation of creatine monohydrate on body composition and strength. Journal of the International Society of Sports Nutrition, 10:36. PMID: 23919405
- Avgerinos KI, Spyrou N, Bougioukas KI, Kapogiannis D (2018). Effects of creatine supplementation on cognitive function of healthy individuals: a systematic review of randomized controlled trials. Experimental Gerontology, 108:166–173. PMID: 29704637
- Smith-Ryan AE, Cabre HE, Eckerson JM, Candow DG (2021). Creatine supplementation in women’s health: a lifespan perspective. Nutrients, 13(3):877. PMID: 33670788
- Poortmans JR, Francaux M (2000). Adverse effects of creatine supplementation: fact or fiction? Sports Medicine, 30(3):155–170. PMID: 10999421
- Kim HJ, Kim CK, Carpentier A, Poortmans JR (2011). Studies on the safety of creatine supplementation. Amino Acids, 40(5):1409–1418. PMID: 21484390
- Hultman E, Söderlund K, Timmons JA, et al. (1996). Muscle creatine loading in men. Journal of Applied Physiology, 81(1):232–237. PMID: 8964750
- Burke DG, Chilibeck PD, Parise G, et al. (2003). Effect of creatine and weight training on muscle creatine and performance in vegetarians. Medicine and Science in Sports and Exercise, 35(11):1946–1955. PMID: 14600563
- Branch JD (2003). Effect of creatine supplementation on body composition and performance: a meta-analysis. International Journal of Sport Nutrition and Exercise Metabolism, 13(2):198–226. PMID: 12701816
- Devries MC, Phillips SM (2014). Creatine supplementation during resistance training in older adults — a meta-analysis. Medicine and Science in Sports and Exercise, 46(6):1194–1203. PMID: 24576864
- Spillane M, Schoch R, Cooke M, et al. (2009). The effects of creatine ethyl ester supplementation combined with heavy resistance training on body composition, muscle performance, and serum and muscle creatine levels. Journal of the International Society of Sports Nutrition, 6:6. PMID: 19228401
- Jagim AR, Oliver JM, Sanchez A, et al. (2012). A buffered form of creatine does not promote greater changes in muscle creatine content, body composition, or training adaptations than creatine monohydrate. Journal of the International Society of Sports Nutrition, 9(1):43. PMID: 22817979
- Van der Merwe J, Brooks NE, Myburgh KH (2009). Three weeks of creatine monohydrate supplementation affects dihydrotestosterone to testosterone ratio in college-aged rugby players. Clinical Journal of Sport Medicine, 19(5):399–404. PMID: 19741313
- Greenwood M, Kreider RB, Melton C, et al. (2003). Creatine supplementation during college football training does not increase the incidence of cramping or injury. Molecular and Cellular Biochemistry, 244(1–2):83–88.
- Gordji-Nejad A, Matusch A, Kleedörfer S, et al. (2024). Single dose creatine improves cognitive performance and induces changes in cerebral high energy phosphates during sleep deprivation. Scientific Reports, 14:4937. PMID: 38388765